ADR Intelligent Reporting System
A medication-safety platform that turns clinical instant messages and hospital-data triggers into reviewable ADR signals, report drafts, and traceable submission workflows.
Clinical problem
ADR evidence is often scattered across messages, laboratory abnormalities, medication orders, and patient narratives. Manual reporting is slow and easy to miss during routine clinical work.
Under-reporting
Fragmented evidence
Manual workload
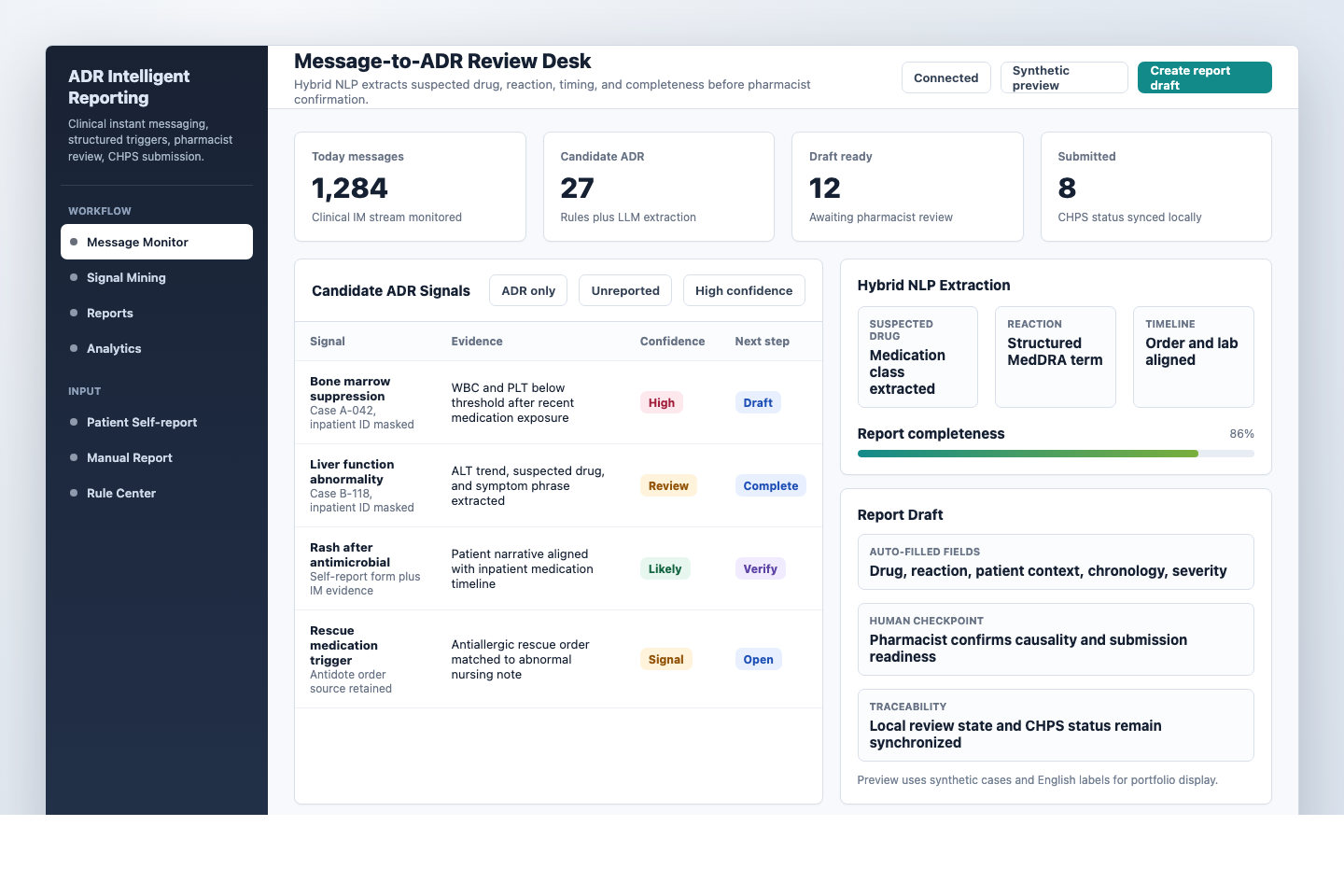
What I built
A workflow for message monitoring, signal mining, patient self-report intake, report management, CHPS status synchronization, and rule-center configuration.
Signal queue
Draft report
CHPS sync
My role
I designed the clinical workflow, data logic, review states, and hybrid NLP pipeline that keeps AI assistance subordinate to pharmacist confirmation.
Clinical design
Hybrid NLP
Human review